(Poster 165) Recurrent Prolapse in Bladder Exstrophy: Balancing Repair and Outcomes
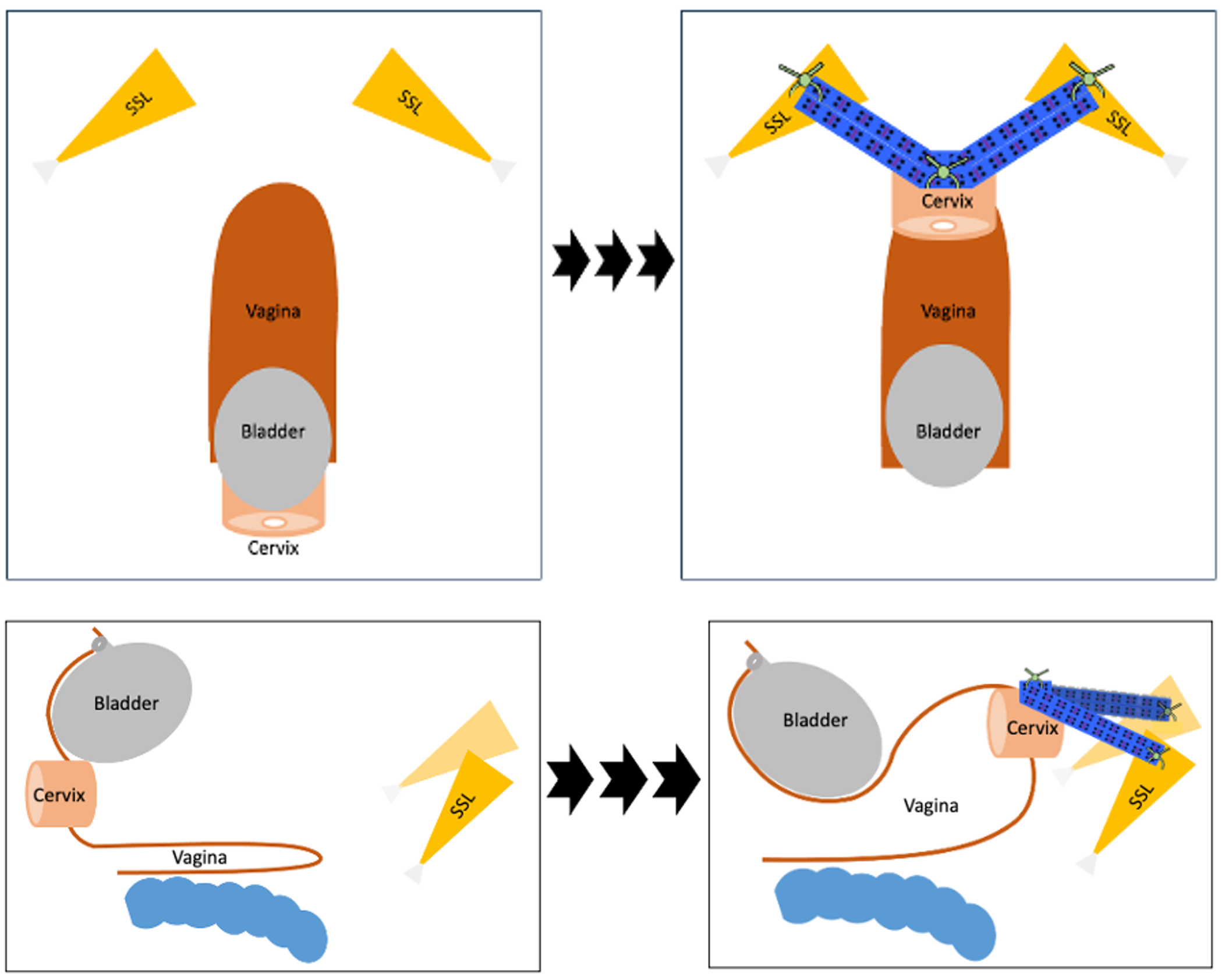
Axial and sagittal views of bilateral sacrospinous hysteropexy with mesh.
Preoperative and postoperative POP-Q Examinations.
Objectives: Bladder exstrophy (BE) is a rare congenital anomaly that is often accompanied by pubic diastasis, anterior displacement of the vagina, and a congenitally weakened pelvic floor. Pelvic organ prolapse is becoming more frequently encountered in women with a history of BE as life expectancy improves. Management of these cases is complex, especially in those with recurrent prolapse.
We report here on the management of recurrent stage III cervical stump and anterior vaginal wall prolapse in a patient with BE and prior sacrocolpopexy with one year follow up.
Methods: A 68-year-old female presented with bothersome recurrent pelvic organ prolapse several years after a robotic, converted to open, supracervical hysterectomy, bilateral salpingectomy/oophorectomy, and sacrocolpopexy with her operative report noting severe intra-abdominal adhesive disease. She had a history of BE for which she underwent numerous abdominal and vaginal reconstructive surgeries, including urethral reconstruction. Her medical history was significant for diabetes and class III obesity.
Physical examination revealed an absent pubic symphysis with bony pelvic diastasis and stage III cervical stump and anterior vaginal wall prolapse (Figure 1a).
The patient desired surgical management; however, performing any transabdominal surgery would have an elevated risk of bowel injury and encountering significant adhesions. There was also concern for a fully corrected anterior vaginal wall to unmask stress urinary incontinence (SUI), which would be difficult to manage given her prior urethral reconstruction. The goal was to correct her apical prolapse and avoid extensive repair in a previously operated anterior vaginal wall. A plan was made for a bilateral sacrospinous ligament hysteropexy through an anterior dissection using a customized mesh strip.
Intraoperatively, a customized rectangular polypropylene mesh was made from the apical arm of a sacrocolpopexy mesh. Polypropylene sutures were placed in the bilateral sacrospinous ligaments and were threaded through the ipsilateral mesh corners with the midline of the mesh sutured to the subepithelial anterior portion of the cervix.
With tying the sutures and elevating the mesh to the sacrospinous ligaments, good apical support was seen with a remaining stage 2 cystocele (Figure 2).
Results: At one year postoperatively, the patient remained asymptomatic from any prolapse symptoms. Her POP-Q (Figure 1b) revealed a remaining stage III cystocele with resolved cervical stump prolapse. She had initial SUI in the first week post-operation which resolved by her 6-week postoperative visit.
Conclusions: Patients with BE present unique challenges for pelvic organ prolapse surgeons. Achieving the most appropriate symptom relief requires balancing anatomic correction with patient-centered goals and patient-specific risks, aiming to restore function without introducing new complications.

.png)
